Controversy continues to surround the optimal approach to managing postoperative nausea and vomiting (PONV)
1. In a recent article, Scuderi et al 2 reported that routine antiemetic prophylaxis with ondansetron, 4 mg IV, given before the start of surgery did not result in a clinically important improvement in patient outcome compared with symptomatic treatment. In an accompanying editorial, Fisher 3 stated, “there appears to be little evidence to support routine prophylactic administration of antiemetics.” While this may be true for patients at low-risk (<5%) of developing emetic symptoms, higher risk patient populations clearly benefit from the use of prophylactic approaches to minimize the uncomfortable symptoms of nausea and vomiting 4-5. In a more recent study, Scuderi and colleagues 6 found that prophylaxis resulted in an increased level of patient satisfaction compared to systematic treatment in women undergoing outpatient laparoscopic surgery.In spite of the routine use of prophylactic antiemetic drugs in patients at increased risk to developing emetic symptoms, a surprising number of these patients will still require a “rescue” therapy. In a systematic review of postoperative vomiting after day-case surgery, McQuay and Moore 6B concluded that none of the currently available antiemetic drugs are sufficiently effective to be used for routine prophylaxis. When patients develop nausea and vomiting despite pharmacologic prophylaxis, consideration should be given to the use of complimentary non-pharmacologic and other novel therapies 7. Some of the novel pharmacologic therapies include neurokinin-1 (NK-1) antagonists and inhaled isopropyl alcohol. A wide variety of non-pharmacologic approaches have also been reported to be effective in the prevention of nausea and vomiting including acupuncture 8, electroacupuncture 9, transcutaneous electrical acupoint stimulation 10-12, and acupressure 13-16. In addition to the Sea BandTM acupressure device, a commercially available acupoint stimulating device (known as a ReliefBand®) has recently received FDA-approval for use as an adjuvant to standard pharmacological approaches for treating nausea and vomiting. Acustimulation would appear to be useful alternative to standard antiemetic drugs both as a “rescue” therapy when conventional prophylactic antiemetics proved to be inadequate, and as an adjunctive prophylactic treatment in higher risk patient populations.
Defining Emetic Symptoms
Prior to examining the evidence supporting the use of these novel antiemetic therapies in the management of nausea and vomiting (or retching), it is important to clarify the terminology used to describe these symptoms. Nausea is defined as a subjectively unpleasant sensation associated with awareness of the urge to vomit. It is usually felt in the back of the throat and epigastrium, and is accompanied by the loss of gastric tone, duodenal contractions, and reflux of the intestinal contents into the stomach 17. Retching is defined as labored, spasmodic, rhythmic contractions of the respiratory muscles including the diaphragm, chest wall, and abdominal wall muscles without the expulsion of gastric contents 18. Vomiting, or emesis, is the forceful expulsion of gastric contents from the mouth and is brought about by the powerful sustained contraction of the abdominal muscles, descent of the diaphragm, and opening of the gastric cardiac 19.
Factors Associated with Nausea and Vomiting
Factors which are known to influence the frequency of emetic symptoms include the patient profile, the nature of their underlying disease, pregnancy, the type of operation, as well as anesthetic, analgesic and chemotherapeutic drugs. The well-known patient-related factors include age (young > old), gender (women > men), body habitus (obesity), gastroparesis (diabetics), history of motion sickness or previous postoperative or pregnancy-related nausea and vomiting, smoking history and level of anxiety 20. In the perioperative period, both anesthetic and surgical related factors, as well as patient factors, can contribute to PONV (Table 1). Apfel et al 21-22 identified female gender, nonsmoking status, history of PONV or motion sickness, and the postoperative use of opioids as risk factors.
A simplified risk scoring system provides better discrimination and calibration properties than the more complex risk scores 22B- 22C. The presence of none, one, two, three, or four of these factors was associated with a risk for PONV of 10, 21, 39, 61, and 79%, respectively. Sinclair et al 23 noted that age, type of surgery, and duration and type of anesthesia were additional independent risk factors.
The risk of PONV is highest when susceptible patients (e.g., females, non-smokers, with a history of motion sickness and/or PONV undergo emetogenic surgical procedure under general anesthesia with opioids and inhaled anesthetics.
Non-Pharmacologic Therapies
Acupuncture
In a pilot study evaluating the use of acupuncture for the prophylactic treatment of migraine headache, Lenhard and Waite 24 observed that the attacks were “less severe and less often accompanied by nausea and vomiting.
” Subsequently, Dundee and colleagues 25 performed a sham-controlled study to evaluate the use of traditional Chinese acupuncture in patients undergoing minor gynecologic surgical procedures. In this preliminary study 25, they concluded that manual needling for 5 min at the P6 (Neiguan) acupoint significantly reduced perioperative nausea and vomiting. In a follow-up study, Ghaly et al 26 reported that low frequency (10 Hz) electrical stimulation at the P6 acupoint was as effective as manual needling in reducing the incidence of PONV for 6 h after the operation.
Although acustimulation using locally applied pressure was less effective than acupuncture during the initial 1-6 h study period 27, it was alleged to be as effective as standard antiemetic drugs. When the P6 acupoint was infiltrated with 1% lidocaine, it appeared to block the acupuncture-induced antiemetic activity 28.
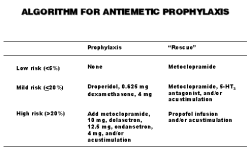
Fig. 1: An algorithm for the treatment and prevention of nausea and vomiting.
A more recent study 29 involving women undergoing outpatient laparoscopic surgery reported that acupuncture reduced PONV from 65% to 35% before and from 60% to 31% after discharge compared to placebo (“sham”) treatment. Somri and colleagues 29B have compared P6 acupuncture to ondansetron (150 μg/kg IV) in a placebo-controlled study involving children undergoing dental surgery. Compared to the placebo group, fewer patients in the acupuncture and ondansetron group vomited and parental satisfaction scores were also higher. However, a recent sham-controlled study by Rusy and colleagues 29C involving children undergoing tonsillectomy with or without adenoidectomy found that electroacupuncture at the P6 site reduced postoperative nausea but did not significantly reduce the incidence or number of pisodes of emesis or the need for rescue antiemetics. These authors suggested that the efficacy of P6 acupuncture for the prevention of PONV was similar to commonly used pharmacotherapies.
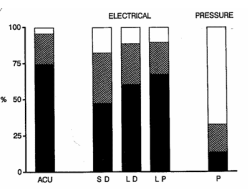
Dundee et al also found that acupuncture possessed significant antiemetic activity in patients receiving chemotherapy 30. Although the antiemetic effect produced by electrical stimulation (10 Hz) of the P6 acupoint lasted only 6-8 h, Dundee and Yang 31 found that P6 acupressure could prolong the antiemetic action of acupuncture for 24 h in patients receiving cancer chemotherapy. In cancer patients experiencing chemotherapy-induced emetic symptoms despite the administration of standard antiemetic drugs, the use of P6 acupuncture combined with 5 min of transcutaneous electrical acupoint stimulation at 2 hr intervals using low impedance electrodes provided significant relief from their symptoms (Fig. 2) 32.
Aglietti et al also reported that P6 acupuncture decreased the intensity and duration of chemotherapyinduced nausea and vomiting in women treated with cisplatin when administered as part of a “multimodal” approach utilizing standard antiemetics, dexamethasone and acupuncture 33.
Fig. 2: Comparative effects of acupuncture (ACU), transcutaneous acupoint electrical stimulation (TAES), and acupressure (AP) when administered at the P6 location by a medical doctor (D) or the patient (P) using small (S) or large (L) cutaneous electrode pads. Frequency of good (ν), slight (��) or no relief (��) of chemotherapy-induced emetic symptoms (Dundee et al, 1991) (32).
Recently, Kotani and colleagues
33B found that preoperative placement of small intradermal needles at dermatomal levels corresponding to the surgical incision reduced both postoperative pain and emetic symptoms. Carlsson et al 34 found that manual acupuncture also reduced hyperemesis gravidarum. This cross-over study reported that active (deep) P6 acupoint stimulation was more effective than “superficial” stimulation in stopping pregnancy-induced nausea. In children undergoing tonsillectomy procedures, postoperative acupuncture (even when combined with preoperative acupressure) failed to prevent emetic symptoms 35. Moreover, it must be acknowledged that acupuncture is an invasive procedure which can produce local (e.g., erythema, hematomas) and even systemic (e.g., acute intracranial hemorrhage) complications 35-36.Acupressure
Dundee and his colleagues were among the first to demonstrate the antiemetic efficacy of P6 acupressure 37. Barsoum et al 38 found that acupressure using an elastic wrist band containing a plastic button (SeaBandTM) reduced the severity of postoperative nausea.
Although the incidence of postoperative vomiting was also reduced, the difference was not statistically significant 38. Similarly, Shyr et al 39 found that injection of 3 ml of saline at the P6 acupoint appeared to reduce PONV. While Allen et al 40 failed to find that P6 acupressure reduced the incidence of PONV, it did decrease the need for “rescue” antiemetic drugs after major gynecologic surgery. Prophylactic application of bilateral acupressure bands at the P6 acupoint reduced nausea and vomiting related to epidural morphine after cesarean delivery 41. Stein et al 14 reported that acupressure was as effective as metoclopramide in preventing nausea and vomiting during spinal anesthesia for cesarean delivery.
Harmon et al 41 similarly found that P6 acupuncture reduced the incidence of nausea and vomiting from 53 to 23% during and from 66 to 36% after cesarean delivery.
In a sham-controlled study involving outpatients undergoing short ambulatory surgery procedures, Fan et al 15 reported that prophylactic bilateral P6 acupressure reduced PONV from 41% to 23%. Although there appears to be a significant “placebo” effect associated with acupressure 42, it reduced PONV in the stepdown (Phase II) recovery unit from 50% (control) to 20% and 10% in the “sham” and active treatment groups, respectively. A more recent study involving women undergoing brief gynecologic surgery procedures 43, the investigator found that “sham” (nonacupoint) stimulation decreased vomiting, but only active P6 stimulation decreased vomiting and the need for rescue antiemetic drugs. Harmon et al 44 reported that acupressure reduced PONV from 42 to 19% compared to placebo after outpatient laparoscopy. In a placebo and sham-controlled study, Agarwal and colleagues 44B reported that P6 acupressure applied 30 min prior to induction of anesthesia reduced PONV and the need for “rescue” antiemetics comparably to ondansetron 4 mg IV in patients undergoing laparoscopic cholecystectomy procedures. However, Agarwal et al 45 failed to demonstrate a decrease in the incidence of PONV after outpatient endoscopic urologic procedures despite the application of bilateral wristbands at the P6 acupoint for 30 min before induction of general anesthesia. Another study involving postsurgical patients at increased risk of PONV failed to find a significant antiemetic effect after unilateral or bilateral application of the SeaBand 45B. However, the authors cautioned that the power analysis suggested that the group sizes were inadequate.
In a sham-controlled study, P6 acupressure reduced symptoms of nausea, but not the frequency of vomiting in pregnant women 46. However, Werntoft and Dykes 46B reported that P6 acupressure reduced nausea and vomiting during pregnancy compared to “sham” acupressure (at a “placebo” point) and to no treatment. Stainton and Neff 47 also found that acupressure with a SeaBandTM reduced nausea and vomiting in pregnancy by 50% if applied “early in the symptom experience.”
Steele et al 47B studied bilateral P6 acupressure using a sham-controlled, cross-over study design and concluded that the SeaBandTM was “a non-invasive, inexpensive, safe and effective treatment for the nausea and vomiting of pregnancy.
In a recent review article by Roscoe and Matteson 47C, these authors suggested that Neiguan-point stimulation using the wrist band is efficacious for relief of nausea associated with pregnancy.
A recent sham-controlled study by Boehler and colleagues 47D reported that Korean hand acupressure applied at point K-K9 for 24 h prior to surgery significantly reduced nausea (40% vs 705) and vomiting (22% vs 50%) in women undergoing minor gynecologic laparoscopic surgery under general anesthesia.
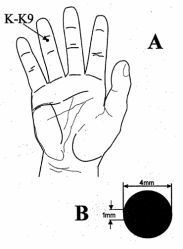
In children, bilateral P6 acupressure failed to reduce the evidence of postoperative vomiting in children undergoing strabismus surgery 48. However, bilateral acupressure using the “vital point” needless acuplaster (Koa, Japan) applied at BL-10, BL-11 and GB-34 acupoints the night before strabismus correction surgery reduced postoperative vomiting from 36 to 15% in the early phase of recovery and from 58 to 24% during the late recovery phase compared to placebo, respectively 49. In a recent study involving children undergoing strabismus surgery 16, Korean hand acupressure at the K9 acupoint (Fig. 3) reduced postoperative vomiting from 68% to 20% compared to placebo treatments. Cummings 49B also confirmed that hand acupressure reduced postoperative vomiting after strabismus surgery
Fig. 3: The “AB-Bong” acupressure device applied at the Korean K9 acupoint (16).
Transcutaneous Electrical Acupoint Stimulation
In adults undergoing laparoscopic cholecystectomy procedures, Zarate et al 12 found that TAES stimulation using a commercial device known as a ReliefBand® (Woodside Biomedical, Carlsbad, CA) reduced the incidence and severity of postoperative nausea compared to a “sham” treatment group.
Although the incidence of vomiting was reduced in the TAES group, the difference was not statistically significant compared to the placebo (“sham”) treatment group. In this multicenter study, the electrical stimulation was only applied after completion of the operation.
|
Table 1: Common factors associated with nausea, |
|
I. Patient related factors II. Anesthesia-related factors III. Surgery-related factors |
In a recent placebo and “sham” controlled study
51B comparing TAES with the ReliefBand to ondansetron(4 mg IV) as part of a multimodal regimen for the prevention of PONV after outpatient plastic surgery, the efficacy of this non-pharmacologic modality was clearly evident (Table 2). These data also suggested that TAES could enhance the efficacy of the popular 5-HT3 antagonist. When used as a “rescue” therapy for the treatment of PONV after laparoscopic cholecystectomy procedures 51C, TAES was somewhat les effective than ondansetron (4 mg IV). Furthermore, the combination of TAES and ondansetron was significantly more effective than the non-pharmacologic therapy alone (Table 3).Based on earlier findings from acupuncture and acupressure PONV studies, it would be advisable to also administer prophylactic treatment with TAES before induction of anesthesia when using this modality in the perioperative period.
|
Table 2: Comparative acquisition (direct) costs of commonly used antiemetic drugs and non-pharmacologic acustimulation devices in US dollars (USD) (72). | |
|
|
Cost (USD) |
|
Antiemetic drugs |
|
|
dexamethasone (DecadronÔ), 4 mg |
|
|
dolasetron (AnzemetÔ), 12.5 mg |
|
|
droperidol (InapsineÔ), 0.625 mg |
|
|
metoclopramide (ReglanÔ), 10 mg |
|
|
ondansetron (ZofranÔ), 4 mg |
|
|
Acustimulation devices |
|
|
acupressure (SeaBandÔ) |
|
|
TAES (ReliefBand®) |
|
|
disposable model |
|
|
reusable model |
|
TAES=transcutaneous acupoint electrical stimulation
In children undergoing ambulatory surgery, TAES at both the P6 acupoint was not found to be effective in reducing postoperative vomiting
52. Interestingly, low-level Yag laser stimulation applied to the P6 acupoint for 15 min before and after general anesthesia reduced the incidence of postoperative vomiting in children undergoing strabismus surgery from 85 to 25% compared to a placebo treatment 53. In a pilot study involving women 54, TAES with the ReliefBand® was reported to be effective in suppressing pregnancy-induced nausea and vomiting (87% experienced improvement compared to 43% with a sham device).The ReliefBand® was also reported to be an effective adjunct to standard antiemetic drugs for decreasing the severity of nausea induced by cisplatin-based chemotherapy 55. Finally, in a preliminary crossover study involving adults experiencing seasickness, TAES with the ReliefBandTM was effective in providing relief from their emetic symptoms 56.
Other novel antiemetic therapies
Inhaled isopropyl alcohol has been suggested as a potentially useful therapeutic modality for the treatment of established PONV 56B-56C-56D.
In a preliminary study involving patients who developed PONV in the early postoperative period after general anesthesia, Merritt and colleagues 56C reported that inhalation of isopropyl alcohol was as effective for “rescue” treatment as standard antiemetic drugs. However, in children experiencing PONV after elective outpatient surgery, repetitive inhales isopropyl alcohol only produced a transient benefit compared to inhaled saline. Clearly, further controlled studies are necessary to establish the role of this antiemetic treatment modality.
Another novel pharmacologic modality involves the use of neurokinin-1 (NK-1) antagonist drugs. These unique compounds (e.g., GR-205171; CJ-11,974; CP-122,721; L-754,030 and MK-869) and known to inhibit the effects of substance P in brainstem regions associated with emesis. A prodrug (L-758,298) for the selective neurokinin-1 antagonist L-754,030 was found to possess superior anti-nausea and longer lasting antiemetic properties compared to ondansetron 56E. The active NK-1 antagonist L-754,030 also prevented delayed emesis after chemotherapy 56F. The antiemetic efficacy of the NK-1 antagonists are improved when combined with a 5-HT3 antagonist and dexamethasone 56F, 56G, 56H. However, the NK-1 antagonist MK-869 plus dexamethasone was less efficacious than the 5-HT3 antagonist granisetron plus dexamethasone in controlling acute emesis 56G.
In women under major gynecologic surgery, the NK-1 antagonist GR-205171 was effective in the treatment of established PONV without producing any adverse side effects 57 The NK-1 antagonist CP- 122,721 was compared to ondansetron when administered alone or in combination for the prevention of PONV after lower abdominal procedures in women 58. Oral CP-122,721 decreased the number of emetic episodes during the first 24 h compared with ondansetron. The NK-1 antagonist also enhanced the antiemetic efficacy of the 5-HT3 antagonist when the combination was administered for antiemetic prophylaxis 58.
Summary
While potentially more effective antiemetic drugs are currently undergoing clinical investigation 57-58, these drugs also possess side effects (e.g., headaches) and are typically less effective in controlling the uncomfortable sensation of nausea. The usefulness of a simple, inexpensive, noninvasive device for the treatment and prevention of nausea and vomiting should not be overlooked as practitioners continue to search for more cost-effective approaches to improving patient comfort after surgery, chemotherapy and during pregnancy.
Although there is no proven mechanism to explain the efficacy of acupressure stimulation in reducing nausea and vomiting, it has been previously demonstrated that acupoint stimulation using a transcutaneous electrical nerve stimulation device can increase levels of endogenous analgesic-like substances within the central nervous system 59.
More than 25 years ago, Anderson and Krohg 60 demonstrated that the relief of pain led to the resolution of emetic symptoms in over 80% of patients experiencing both pain and nausea in the early postoperative period.
Future studies involving acupoint stimulation should carefully examine the relationship between pain and emesis. While many practitioners still consider nausea and vomiting to be a “minor” complication associated with anesthesia and surgery, it remains “a big, ‘little’ problem” 61 for many of our patients.
Concerns regarding the side effects associated with traditional antiemetics (e.g., dysphoria, restlessness and drowsiness with droperidol, extrapyramidal reactions to metoclopramide, and headaches with the 5- HT3 antagonists) 20, have led many practitioners to consider the use of novel pharmacologic agents and complimentary nonpharmacologic techniques for the management of emetic symptoms 7. Recently, the most cost-effective antiemetic drug, droperidol, has been issued a “Black Box” warning by the FDA because of concerns regarding the potential for serious pro-arrhythmogenic effects and even death after low doses of the popular antiemetic 61B. Although most experts in the field have questioned the FDA’s action, many hospital Pharmacy & Therapeutic Committees in the USA have decided to remove droperidol from their formularies 61C. Furthermore, since single drug prophylaxis is associated with a high failure rate in “at risk” populations 62, consideration should be given to combining pharmacologic and nonpharmacologic approaches to eliminating the uncomfortable symptoms of nausea and vomiting. For patients who have received antiemetic prophylaxis, both Scuderi et al 2 and Hill et al 63 have found that administering a second dose of the same antiemetic is often ineffective. In this situation, the use of a novel (e.g., isopropyl alcohol) or nonpharmacologic treatment modality (e.g., acupressure, TAES) may be a more cost-effective alternative (Fig. 1). Studies involving the use of music and therapeutic suggestions have failed to demonstrate a benefit in reducing nausea and vomiting 63B.
Nausea and vomiting are the most common symptoms experienced in early pregnancy, affecting between 70 and 85% of women. Severe intractable vomiting (or hyperemesis gravidarum) develops in about 1-% of all pregnancies. For the woman and her unborn child, having a “drug-free,” non-invasive approach to controlling nausea and vomiting in pregnancy (e.g., SeaBandTM, ReliefBand®) could offer significant advantages over antiemetic drugs alone. Recent surveys 64 suggest that parturients are increasingly turning to these complementary therapies for managing their emetic symptoms. However, it is clear that more well-controlled clinical trials are needed to establish the cost-benefit ratios for many of these nonpharmacologic alternative (or complementary) therapies 65.
Despite improvements in antiemetic drug therapy, 20-30% of surgical patients 66 and up to 60% of cancer patients 67 still experience nausea and vomiting. According to the findings presented at the NIH Consensus Conference 68, acustimulation (e.g., acupuncture, acupressure, TAES) has been found to be efficacious in the treatment of postoperative, pregnancy, and chemotherapy-induced nausea and vomiting.
Although the clinical relevance of meta-analyses (or systematic literature reviews) in enhancing our understanding of therapies for nausea and vomiting has been questioned 69, the recent analyses by Lee and Done 70 suggests that by using non-pharmacologic techniques, 20-25% of adults will not have early PONV compared to no prophylactic treatment.
Furthermore, these investigators concluded that non-pharmacologic techniques were equivalent to commonly used antiemetic drugs in preventing nausea and vomiting within 6 hr after surgery. However, additional studies which are adequately powered and placebo-controlled are clearly needed 71.
All future studies involving noninvasive acustimulation techniques should include a sham (or placebo) group that receives the same type and intensity of stimulation at a comparable “nonacupoint” location. In comparing acustimulation to the commonly used prophylactic antiemetic drugs, it would be very useful to also include a pharmacoeconomic analysis 72 (Table 4). Recent studies have suggested that a smalldose of droperidol (0.625-1.25 mg IV) is more cost-effective than ondansetron, 4 mg IV, or metoclopramide, 10 mg IV, for routine prophylactic antiemetic therapy (64,73,74). However, the costeffectiveness of prophylactic antiemetic therapy is dependent upon the underlying incidence of PONV, as well as by the dose and the timing of the antiemetic’s administration 75-77, as well as the type of surgical procedure 20.
The role of acustimulation in the prevention and treatment of nausea and vomiting will depend on the results of outcome studies which demonstrate not only reductions in emetic symptoms but more importantly, improvements in patient satisfaction. Although P6 acupuncture stimulation appears to be an effective antiemetic technique (except when administered under general anesthesia) 78, it is an “invasive” procedure which is more costly to administer to patients. Future cost-benefit analysis involving these nonpharmacologic modalities should examine their use as a “rescue” therapy, as well as a complementary therapy in combination with traditional antiemetic drugs for both the treatment and prevention of nausea and vomiting.
Referentes
1. White PF, Watcha MF. Postoperative nausea and vomiting: Prophylaxis versus treatment. Anesth Analg 1999; 89: 1337-9.
2. Scuderi PE, James RL, Harris L, et al. Antiemetic prophylaxis does not improve outcomes after outpatient surgery when compared to symptomatic treatment. Anesthesiology 1999; 90: 360-71.
3. Fisher DM. Surrogate outcomes: meaningful not! Anesthesiology 1999; 90: 355-6.
4. Tang J, Watcha MF, White PF. A comparison of costs and efficacy of ondansetron and droperidol in patients undergoing radical mastectomy. Anesth Analg 1996; 83: 304-13.
5. Sadhasivam S, Saxena A, Subramniam K, et al. Safety and efficacy of prophylactic ondansetron in patients undergoing radical mastectomy. Anesth Analg 1996; 89: 1340-6.
6. Scuderi PE, James RL, Harris L, et al. Multimodal antiemetic management prevents early postoperative vomiting after outpatient laparoscopy. Anesth Analg 2000; 91: 1408-14.
7. White PF. Are nonpharmacologic techniques useful alternatives to antiemetic drugs for the prevention of nausea and vomiting? Anesth Analg 1997; 84: 712-4.
8. Dundee JW, Milligan KR. Acupuncture as an antiemetic. Br Med J 1988; 296: 135-7.
9. Ho RT, Jawan B, Fung ST, et al. Electro-acupuncture and postoperative emesis. Anaesthesia 1990; 45: 327-9.
10. Fassoulaki A, Papilas K, Sarantapoulos C, et al, Transcutaneous electrical nerve stimulation reduces the incidence of vomiting after hysterectomy. Anesth Analg 1993; 76: 1012-4.
11. Yang LC, Jawan B, Chen CN, et al. Comparison of P6 acupoint injection with 50% glucose in water and intravenous droperidol for prevention of vomiting after gynecological laparoscopy. Acta Anaesthesiol cand 1993; 37: 192-4.
12. Zarate E, Mingus M, White, PF, et al. The use of transcutaneous acupoint electrical stimulation for preventing nausea and vomiting after laparoscopic surgery. Anesth Analg 2001; 92: 629-35.
13. Dundee JW, Ghaly RG, Bill KM, et al. Effect of stimulation of the P6 antiemetic point on postoperative nausea and vomiting. Br J Anaesth 1989; 63: 612-8.
14. Stein DJ, Birnbach DJ, Danzer BI, et al. Acupressure versus intravenous metoclopramide to prevent nausea and vomiting during spinal anesthesia for cesarean section. Anesth Analg 1997; 84: 342-5.
15. Fan CF, Tanhui E, Joshi S, et al. Acupressure treatment for prevention of postoperative nausea and vomiting. Anesth Analg 1997; 84: 821-5.
16. Schlager A, Boehler M, Puhringer F. Korean hand acupressure reduces postoperative vomiting in children after strabismus surgery. Br J Anaesth 2000; 85: 267-70.
17. Stein JM. Factors affecting nausea and vomiting in the plastic surgery patient. Plast Reconstr Surg 1982; 70: 505-11.
18. Seigel LJ, Lomgo DL. The control of chemotherapy-induced emesis. Ann Intern Med 1981; 95: 352-9.
19. Bellville JW, Bross IDJ, Howland WS. Postoperative nausea and vomiting IV: Factors related to postoperative nausea and vomiting. Anesthesiology 1960; 21: 186-93.
20. Watcha MF, White PF. Postoperative nausea and vomiting. Its etiology, treatment and prevention. Anesthesiology 1992; 77: 162-84.
21. Apfel CC, Greim CA. Haubitz I, et al. The discriminating power of a risk score for postoperative vomiting in adults undergoing various types of surgery. Acta Anaesthesiol Scand 1998; 42: 502-9.
22. Apfel CC, Laara E, Koivuranta M, et al. A simplified risk score for predicting postoperative nausea and vomiting. Conclusions from cross-validations between two centers. Anesthesiology 1999; 91: 693-700.
23. Sinclair DR, Chung F, Mezei G. Can postoperative nausea and vomiting be predicted? Anesthesiology 1999; 91: 109-18.
24. Lenhard L, Waite PM. Acupuncture in the prophylactic treatment of migraine headaches: pilot study. N Z Med J 1983; 96: 663-6.
25. Dundee JW, Chestnutt WN, Ghaly RG, et al. Traditional Chinese acupuncture: A potentially useful antiemetic? Br Med J 1986; 293: 583-4.
26. Ghaly RG, Fitzpatrick KT, Dundee JW. Antiemetic studies with traditional Chinese acupuncture. A comparison of manual needling with electrical stimulation and commonly used antiemetics. Anaesthesia 1987; 42: 1108-10.
27. Dundee JW, Ghaly RG, Bill KM, et al. Effect of stimulation of the P6 antiemetic point on postoperative nausea and vomiting. Br J Anaesth 1989; 63: 612-8.
28. Dundee JW, Ghaly G. Local anesthesia blocks the antiemetic action of P6 acupuncture. Clin Pharmacol Ther 1991; 50: 78-80.
29. Al-Sadi M, Newman B, Julious SA. Acupuncture in the prevention of postoperative nausea and vomiting. Anaesthesia 1997; 52: 658-61.
30. Dundee JW, Ghaly RG, Fitzpatrick KT, et al. Acupuncture prophylaxis of cancer chemotherapy-induced sickness. J R Soc Med 1989; 82: 268-71.
31. Dundee JW, Yang J. Prolongation of the antiemetic action of P6 acupuncture by acupressure in patients having cancer chemotherapy. J R Soc Med 1990; 83: 360-2.
32. Dundee JW, Yang J, McMillan C. Non-invasive stimulation of the P6 antiemetic acupuncture point in cancer chemotherapy. J R Soc Med 1991; 84: 210-2.
33. Aglietti L, Roila F, Tonato M, et al. A pilot study of metoclopramide, dexamethasone, diphenhydramine and acupuncture in women treated with cisplatin. Cancer Chemother Pharmacol 1990; 26: 239-40.
34. Carlsson CP, Axemo P, Bodin A, et al. Manual acupuncture reduces hyperemesis gravidarum. A placebocontrolled, randomized, single-blind, crossover study. J Pain Symptom Manage 2000; 20: 273-9.
35. Shenkman Z, Holzman RS, Kim C, et al. Acupressure-acupuncture antiemetic prophylaxis in children undergoing tonsillectomy. Anesthesiology 1999; 90: 1311-6.
36. Choo DC, Yue G. Acute intracranial hemorrhage caused by acupuncture. Headache 2000; 40: 397-8.
37. Dundee JW, Sourial FB, Ghaly RG, et al. P6 acupressure reduces morning sickness. J R Soc Med 1988; 71: 456-7.
38. Barsoum G, Perry EP, Fraser IA. Postoperative nausea is relieved by acupressure. J R Soc Med 1990; 83: 86-9. 39. Shyr MH, Hsu JC, Wu YW, et al. P6 acupoint injection reduced postoperative nausea and vomiting. Ma Tsui Hsueh Tsa Chi 2000; 28: 357-60.
40. Allen DL, Kitching AJ, Nagle C. P6 acupressure and nausea and vomiting after gynaecological surgery. Anaesth Intensive Care 1994; 22: 691-3.
41. Harmon D, Ryan M, Kelly A, et al. Acupressure and prevention of nausea and vomiting during and after spinal anaesthesia for cesarean section. Br J Anaesth 2000; 84: 463-7.
42. Ferrara-Love R, Sekeres L, Bircher NG. Nonpharmacologic treatment for postoperative nausea. J Perianesth Nurs 1996; 11: 78-83.
43. Alkaissi A, Stalnert M, Kalman S. Effect and placebo effect of acupressure (P6) on nausea and vomiting after outpatient gynaecological surgery. Acta Anaesthesiol Scand 1999; 43: 270-4.
44. Harmon D, Gardiner J, Harrison R, et al. Acupressure and the prevention of nausea and vomiting after laparoscopy. Br J Anaesth 1999; 82: 387-90.
45. Agarwal A, Pathak A, Gaur A. Acupressure wristbands do not prevent postoperative nausea and vomiting after urological endoscopic surgery. Can J Anaesth 2000; 47: 319-24.
46. Belluomini J, Litt RC, Lee KA, et al. Acupressure for nausea and vomiting of pregnancy: A randomized, blinded study. Obstet Gynecol 1994; 84: 245-8.
47. Stainton MC, Neff EJ. The efficacy of SeaBands for the control of nausea and vomiting in pregnancy. Health Care Women Int 1994; 15: 563-75.
48. Lewis IH, Pryn SJ, Reynolds PI, et al. Effect of P6 acupressure on postoperative vomiting in children undergoing outpatient strabismus correction. Br J Anaesth 1991; 67: 73-8.
49. Chu YC, Lin SM, Hsieh YC, et al. Effect of BL-10 (tianzhu), BL-11 (dazhu) and GB-34 (yanglinquan) acuplaster for prevention of vomiting after strabismus surgery in children. Acta Anaesthesiol Sin 1998; 36: 11-6.
50. Dundee JW, McMillan CM. Clinical uses of P6 acupuncture and antiemetics. Acupunct Electrother Res 1990; 335: 265-6.
51. Hu S, Stern RM, Koch KL. Electrical acustimulation relieves vection-induced motion sickness. Gastroenterology 1992; 102: 1854-8.
52. Schwager KL, Baines DB, Meyer RJ. Acupuncture and postoperative vomiting in day-stay paediatric patients. Anaesth Intensive Care 1996; 24: 274-7.
53. Schlager A, Offer T, Baldissera I. Laser stimulation of acupuncture point P6 reduces postoperative vomiting in children undergoing strabismus surgery. Br J Anaesth 1998; 81: 529-32.
54. Evans AT, Samuels SN, Marshall C, et al. Suppression of pregnancy-induced nausea and vomiting with sensory afferent stimulation. J Reprod Med 1993; 38: 603-6.
55. Pearl ML, Fischer M, McCauley DL, et al. Transcutaneous electrical nerve stimulation as an adjunct for controlling chemotherapy-induced nausea and vomiting in gynecologic oncology patients. Cancer Nurs 1999: 22: 307-11.
56. Bertolucci LE, DiDario B. Efficacy of a portable acustimulation device in controlling seasickness. Aviat Space Environ Med 1995; 66: 1155-8.
57. Diemunsch P, Schoeffler P, Bryssine B, et al. Anti-emetic activity of the NK-1 receptor antagonist GR 205171 in the treatment of established PONV following major gynecological surgery. Br J Anaesth 1999; 82: 274-6.
58. Gesztesi Z, Scuderi PE, White PF, et al. Substance P (Neurokinin-1) antagonist prevents postoperative vomiting after abdominal hysterectomy procedures. Anesthesiology 2000; 93: 931-7.
59. Han JS, Chen XH, Sun SL, et al. Effect of low- and high-frequency TENS on Met-enkephalin-Arg-Phe and dynorphin A immunoreactivity in human lumbar CSF. Pain 1991; 47: 295-8.
60. Anderson R, Krohg K. Pain as a major cause of postoperative nausea. Can Anaesth Soc J 1976; 23: 366-9.
61. Kapur PA. The big “little” problem (editorial). Anesth Analg 1991; 73: 243-5.
62. Watcha MF. The cost-effective management of postoperative nausea and vomiting. Anesthesiology 2000; 92: 931-3.
63. Hill RP, Lubarsky DA, Phillips-Bute B, et al. Cost-effectiveness of prophylactic antiemetic therapy with ondansetron, droperidol, or placebo. Anesthesiology 2000; 92: 958-67
64. Allaire AD, Moos MK, Wells SR. Complementary and alternative medicine in pregnancy: A survey of North Carolina certified nurse-midwives. Obstet Gynecol 2000; 95: 19-23.
65. Mazzotta P, Magee LA. A risk-benefit assessment of pharmacological and nonpharmacological treatments for nausea and vomiting of pregnancy. Drugs 2000; 59: 781-800.
66. Thompson HJ. The management of post-operative nausea and vomiting. J Adv Nurs 1999; 29: 1130-6.
67. King CR. Nonpharmacologic management of chemotherapy-induced nausea and vomiting. Oncol Nurs Forum 1997; 24: 41-8.
68. NIH Consensus Conference. Acupuncture. JAMA 1998; 280: 1518-24.
69. White PF, Watcha MF. Has the use of meta-analysis enhanced our understanding of therapies for postoperative nausea and vomiting? Anesth Analg 1999; 88: 1200-2.
70. Lee A, Done ML. The use of nonpharmacologic techniques to prevent postoperative nausea and vomiting: A meta-analysis. Anesth Analg 1999; 88: 1362-9.
71. Streitberger K, Kleinhenz J. Introducing a placebo needle into acupuncture research. Lancet 1998; 352: 364-5.
72. Watcha MF, White PF. Economics of anesthetic practice. Anesthesiology 1997; 86: 1170-96.
73. Tang J, Watcha MF, White PF. A comparison of costs and efficacy of ondansetron and droperidol as prophylactic antiemetic therapy for elective outpatient gynecologic procedures. Anesth Analg 1996; 83: 304-13.
74. Watcha MF. Smith I. Cost-effectiveness analysis of antiemetic therapy for ambulatory surgery. J Clin Anesth 1994; 6: 603-6.
75. Tang J, Wang B, White, PF, et al. The effect of timing of ondansetron administration on its efficacy, costeffectiveness, and cost-benefit as a prophylactic antiemetic in the ambulatory setting. Anesth Analg 1998; 86: 274-82.
76. Sun R, Klein KW, White PF. The effect of timing of ondansetron administration in outpatients undergoing otolaryngologic surgery. Anesth Analg 1997; 84: 331-6.
77. Zarate E, Watcha MF, White PF, et al. A comparison of the costs and efficacy of ondansetron versus dolasetron for antiemetic prophylaxis. Anesth Analg 2000; 90: 1352-8.
78. Vickers AJ. Can acupuncture have specific effects on health? A systematic review of acupuncture antiemesis trials. J Royal Soc Med 1996; 89: 303-311.